The condition affecting 1 in 8 women is now officially called polyendocrine metabolic ovarian syndrome (PMOS). Here's why the name change matters, and what it means for the emerging gut-hormone connection.
PCOS Is Now PMOS — and the Name Change Is Long Overdue

Summary
If you or someone you love has been navigating a PCOS diagnosis, you may have felt something was always a little off about the name: polycystic ovary syndrome. A name that pointed to your ovaries, maybe to your cysts, and not much else. A name that led to an exam, a prescription for birth control or metformin, and the implicit message that your hormones were the problem — and there wasn't a whole lot you could do about it.
On May 12, 2026 , an international medical consensus published in The Lancet made it official: PCOS has a new name. After a 14-year process led by Professor Helena Teede of Monash University and 56 academic, clinical, and patient organizations, with input from more than 14,300 patient and professional respondents, the condition is now formally called polyendocrine metabolic ovarian syndrome, or PMOS [1].
Why the name change matters
The name "polycystic ovary syndrome" was always a misnomer. Pathological ovarian cysts aren't a defining feature of the condition. But the name stuck, and in sticking, it shaped how doctors understood, diagnosed, and treated it for decades.
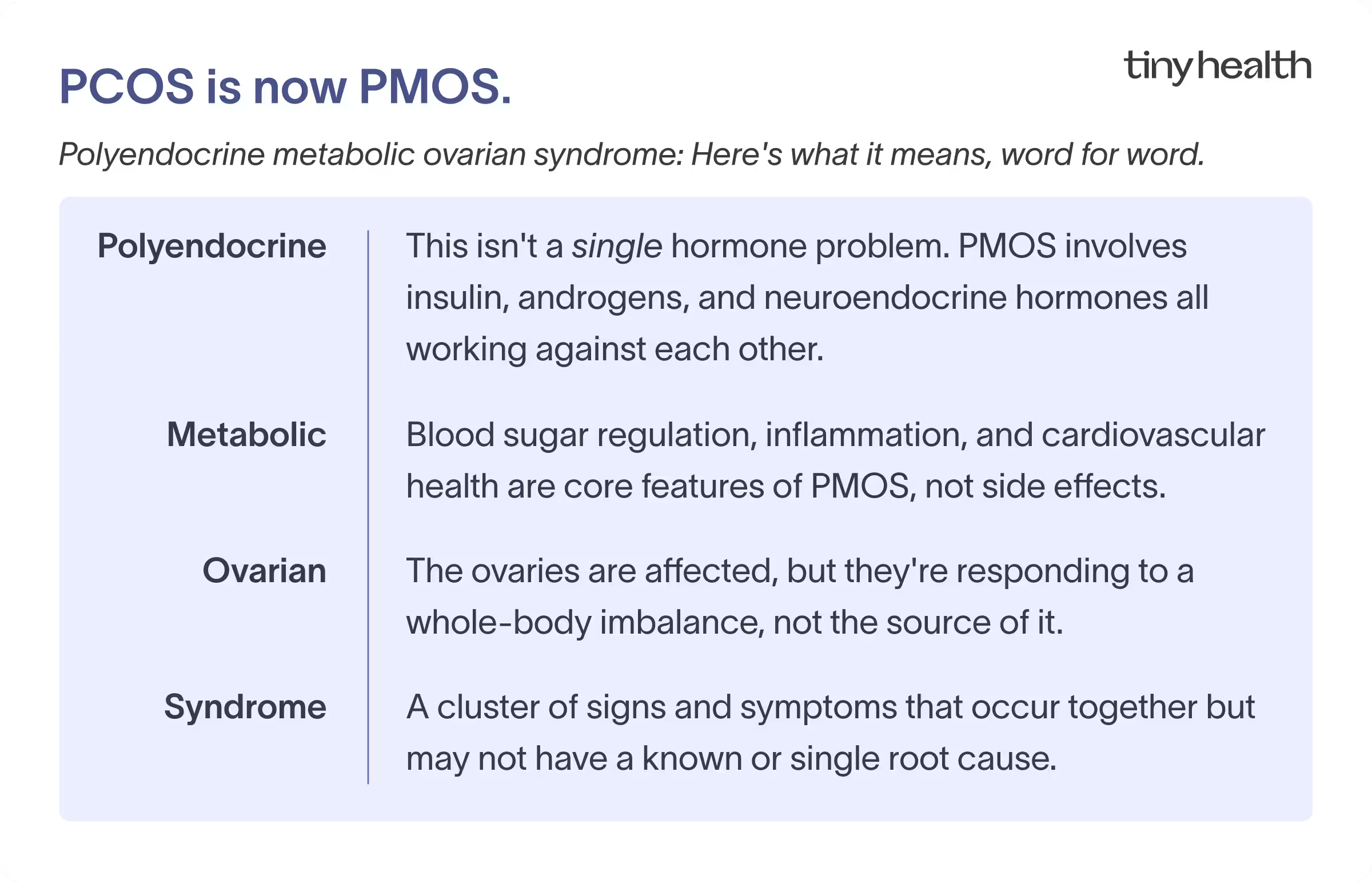
The real picture is far bigger. PMOS involves disturbances across multiple endocrine systems: insulin, androgens, neuroendocrine hormones, and ovarian function. Its features span metabolism (insulin resistance, blood sugar dysregulation, cardiovascular risk), reproduction (irregular cycles, ovulatory dysfunction, fertility challenges), psychology (anxiety, depression, disordered eating), and skin (acne, hair loss, hirsutism). The Lancet paper estimates that up to 70% of people with the condition go undiagnosed. That's not a gap in testing. That's a gap in understanding, and the name contributed to it.
The new name, polyendocrine metabolic ovarian syndrome, acknowledges what the science has been saying for years: this is a multisystem condition rooted in endocrine and metabolic dysfunction. Ovarian involvement is real, but it's part of a broader system.
For the functional medicine community, this moment has been a long time coming. As our Chief Medical Officer, Dr. Elisa Song, put it,
“This is huge. For too long, girls and women have been led to believe this is an ovary problem. PMOS was never just an ovary problem. It's a whole-body condition, and the gut is where the story actually begins.”
The gut is part of this picture
In a 2024 Tiny Health and Mira study of 366 women with PCOS, 94% reported gut health issues.
That's not a coincidence. At Tiny Health, we've written about the gut-hormone connection in PCOS. The science here is still actively evolving, but a clearer picture is forming: PMOS is fundamentally a metabolic and endocrine condition, and the gut sits at the intersection of both.
Here's how the gut microbiome connects to the core features of PMOS:
Insulin resistance and the gut
Insulin resistance is one of the defining metabolic features of PMOS — and importantly, it's not limited to women with overweight or obesity. A 2025 systematic review and meta-analysis estimates prevalence at approximately 75% in lean women with the condition and 95% in those who are overweight or obese [2]. An imbalanced gut microbiome contributes to low-grade inflammation and increased gut permeability (sometimes called leaky gut), which allows bacterial fragments called lipopolysaccharides to enter the bloodstream. This triggers systemic inflammation that worsens insulin resistance [3]. And insulin resistance, in turn, drives the ovaries to produce more androgens, deepening the hormonal disruption at the heart of PMOS.
Androgens and gut bacteria
Elevated androgen levels, the hallmark endocrine feature of PMOS, appear to interact bidirectionally with gut bacteria. An imbalanced microbiome can worsen how the body processes androgens, while androgen excess reshapes the gut environment. Research has identified specific bacterial populations, including Enterococcus, that are more abundant in normal-weight women with PMOS and insulin resistance [4].
Estrogen recycling and the estrobolome
The gut's estrogen-regulating community of microbes, the estrobolome, produces an enzyme called β-glucuronidase that recycles estrogen back into the bloodstream instead of clearing it. In plain English, the gut is doing some of the body's hormone housekeeping, deciding how much keeps circulating versus how much gets cleared out. And in PMOS, that balance is often off. Women with PMOS tend to have higher β-glucuronidase activity, and this enzyme activity correlates with circulating testosterone and estradiol levels — meaning the gut may be amplifying hormonal imbalance from multiple directions, not just through estrogen recycling [5]. This has downstream effects not just on estrogen, but on the broader endocrine environment that PMOS disrupts.
The vaginal microbiome
The gut-vaginal axis is another piece of the PMOS picture that rarely gets attention. Gut dysbiosis can alter the vaginal microbiome, and shifts in vaginal microbial communities have been linked to inflammatory changes that affect reproductive health. For people managing irregular cycles, ovulatory dysfunction, or fertility challenges, this connection matters.
What this means for teen girls
The Lancet consensus makes a point worth emphasizing: PMOS often first appears around puberty. And yet, most adolescents with the condition don't get a diagnosis until years later, if at all. And when they do, options have often been limited to a birth control prescription or metformin.
The new name opens the door to a different conversation. PMOS is not primarily a reproductive condition that girls should have to wait out. It's a metabolic and endocrine condition with roots that show up in the gut, in diet, in inflammation, in stress physiology, all areas where young people have real agency.
It's worth helping teen girls and young women understand that their gut microbiome influences their hormones, that what they eat affects their microbial community in ways that may influence androgen levels and insulin sensitivity, and that the bloating, irregular cycles, acne, and mood swings they're experiencing are signals from a system that can be supported.
Birth control and metformin have their place. But they don't have to be the whole story.
“The girls and young women who learn this — that their gut shapes their hormones, their metabolism, their mood — are empowered to take control of their hormones and have agency over their bodies in a way that our generation never had. That's what this name change makes possible.” - Dr. Elisa Song, CMO
What a systems approach looks like in practice
Renaming PCOS to PMOS is more than semantics. It invites a broader treatment frame, one that asks not just "what organ is the problem?" but "what systems are out of balance, and what can we do across all of them?"
The gut is one of those systems, and it's one you can actively work with. That means looking at things like your β-glucuronidase capacity, your microbial diversity, and how gut inflammation may be interacting with insulin resistance and androgen levels — all of which vary considerably from person to person.
We've covered the practical side of this in depth in our guide to PCOS, hormone balance, and the gut connection, including what the research says about diet, probiotics, and microbiome testing.
Moving forward with PMOS
At Tiny Health, we believe that hormone health shouldn’t be separated from gut health. The gut-metabolic-hormone connection in PMOS is exactly the kind of whole-body picture our tests are built to reveal.
If you or your teenager has PMOS, a gut health test is a concrete starting point. From there, your personalized Action Plan gives you specific recommendations for diet, supplements, and lifestyle based on what's actually going on in your microbiome.
The condition has a new name. The approach to caring for it is evolving too. At the root lies the microbiome.
When to seek medical attention
Reach out to a doctor or specialist if you or your teenager are experiencing:
Signs that may indicate PMOS and warrant evaluation:
- Irregular, infrequent, or absent menstrual cycles, especially if they haven't regulated within two years of a first period
- Significant acne that doesn't respond to standard skincare, particularly along the jawline and chin
- Unusual hair growth on the face, chest, or abdomen, or unexpected hair thinning or loss on the scalp
- Unexplained weight gain or persistent difficulty managing weight despite a balanced diet
- Skin changes such as darkened patches around the neck, armpits, or groin (a sign of insulin resistance called acanthosis nigricans)
- Persistent fatigue, brain fog, or mood symptoms like anxiety and depression that feel tied to your cycle
Seek prompt care if you are:
- Trying to conceive and experiencing irregular cycles or ovulatory dysfunction
- Managing symptoms that are significantly affecting your quality of life, school, work, or mental health
- Already diagnosed with PMOS and noticing your symptoms worsening despite treatment

Trust your gut.
Get to know your microbes with an easy, 5-minute at-home test from Tiny Health. Unlock deep gut health insights and personalized recommendations for your diet, supplements, and lifestyle.

Get Your Personalized Gut Health Plan
Answer a few questions and receive tailored recommendations, plus 20% off

Hannah is a Tiny Health team member, mom of two, and firm believer that quality health information should be accessible to everyone.

Chief Medical Officer
Integrative Pediatrician and Pediatric Functional Medicine Expert
Founder, Healthy Kids Happy Kids
References
[1] H. J. Teede et al., “Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process,” The Lancet, May 2026, doi: 10.1016/S0140-6736(26)00717-8.
[2] C. Zheng et al., “Analyzing and evaluating the metabolic and endocrine characteristics between lean and obese patients with polycystic ovary syndrome: a systemic review and meta-analysis,” Front Endocrinol (Lausanne), vol. 16, p. 1680685, 2025, doi: 10.3389/fendo.2025.1680685.
[3] Y. Sun, S. Gao, C. Ye, and W. Zhao, "Gut microbiota dysbiosis in polycystic ovary syndrome: Mechanisms of progression and clinical applications," Front. Cell. Infect. Microbiol., vol. 13, Feb. 2023, doi: 10.3389/fcimb.2023.1142041.
[4] F. He and Y. Li, “The gut microbial composition in polycystic ovary syndrome with insulin resistance: findings from a normal-weight population,” J Ovarian Res, vol. 14, no. 1, p. 50, Mar. 2021, doi: 10.1186/s13048-021-00799-9.
[5] M. Cai et al., "Characteristics of Gut Microbiota and Its Relationship With Serum Sex Hormones in Non-obese Polycystic Ovary Syndrome Patients With Insulin Resistance," Feb. 02, 2022, Research Square. doi: 10.21203/rs.3.rs-1304673/v1.
[6] J. Patel et al., "Assessment of gut microbial β-glucuronidase and β-glucosidase activity in women with polycystic ovary syndrome," Sci Rep, vol. 13, no. 1, p. 11967, July 2023, doi: 10.1038/s41598-023-39168-5.


